I am a Consultant in Emergency Medicine and Associate Medical Director for Patient Safety and Quality Improvement. I am interested in the application of Ergonomics and Human Factors to various aspects of healthcare, especially designing safer systems.
Photo: D.Stephenson
Final Project
Has the Patient Safety Incident Response Framework led to more system-based investigations and actions?
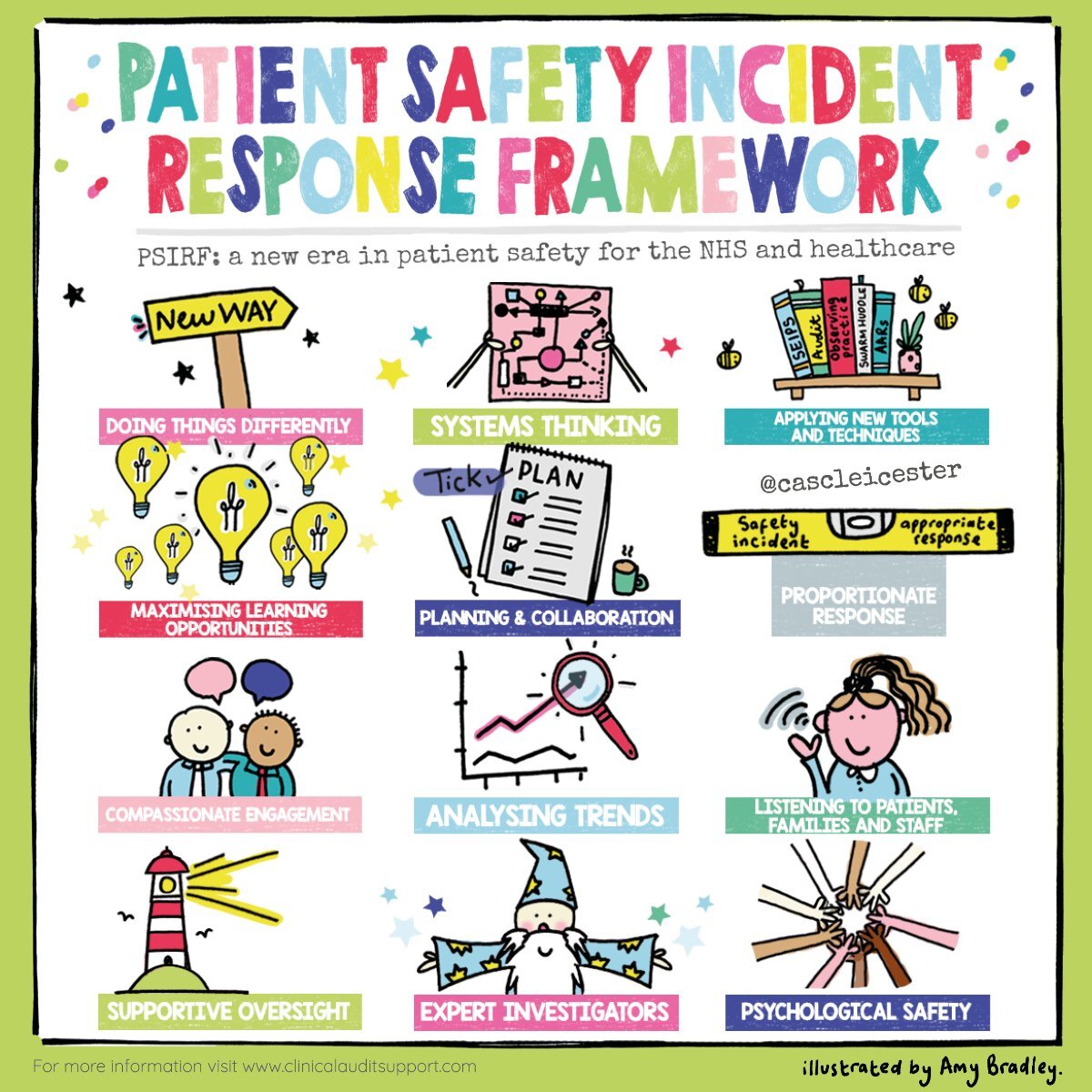
Infographic summarizing the Patient Safety Incident Response Framework (reproduced with permission)
The Patient Safety Incident Response Framework (PSIRF) is a new approach to investigating incidents in the NHS introduced in 2021-2023. It brings a number of changes summarized in the infographic above. My interest was in the impact of the system-based approach.
Objectives: To compare the use of a system-based approach (SBA) in incident investigations and actions before and after the implementation of the Patient Safety Incident Response Framework (PSIRF), using mixed methods.
Methods: The setting was a medium-sized hospital in Northern England.
Quantitative study: Incident reports before (n=20) and after (n=16) PSIRF implementation were analysed using multiple measures of SBA in the investigation and actions.
Qualitative study: Participants were recruited from varied roles who had experience of incident investigation before and after PSIRF implementation (n=10). They were interviewed using a semi-structured approach. Interviews were analysed thematically.
Results:
Quantitative study: There were no significant differences between pre- and post-implementation investigations or actions on overall measures of SBA. However, the median number of contributory factors (CFs) considered in investigations was significantly lower at 2 post-implementation versus 5 pre-implementation (p=0.002).
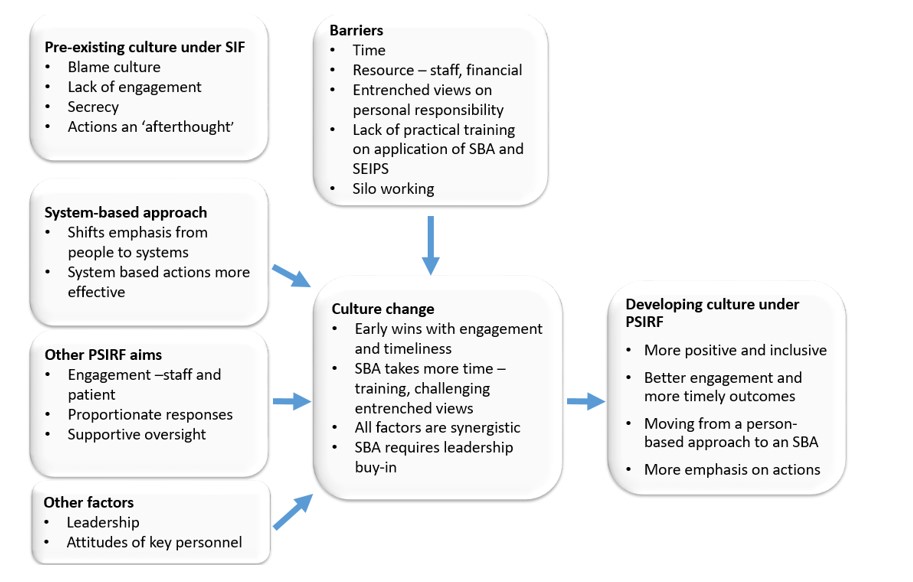
Qualitative study: The over-arching theme was the culture of incident investigation and the change in that culture associated with PSIRF implementation. Subthemes included barriers and facilitators to the uptake of PSIRF and the SBA, the role of the SBA within the culture and the role of SBA in relation to other factors (see thematic map below).
Thematic map of qualitative results
Conclusions: The reduction in CFs under PSIRF was thought to be due to limited uptake of the new guidance on CFs combined with the removal of CFs from the PSIRF investigation templates. Despite the largely non-significant findings of the quantitative study, the qualitative study indicated a complex picture of culture change relating to SBA usage and other factors including increased patient and staff engagement and timeliness of reports. This occurred prior to and during PSIRF implementation, much but not all driven by the implementation itself. Further culture change and greater utilization of the SBA will likely occur with more time and hence the study could be criticized for taking place too soon after implementation.
Other Work
Human Factors and Complex Systems
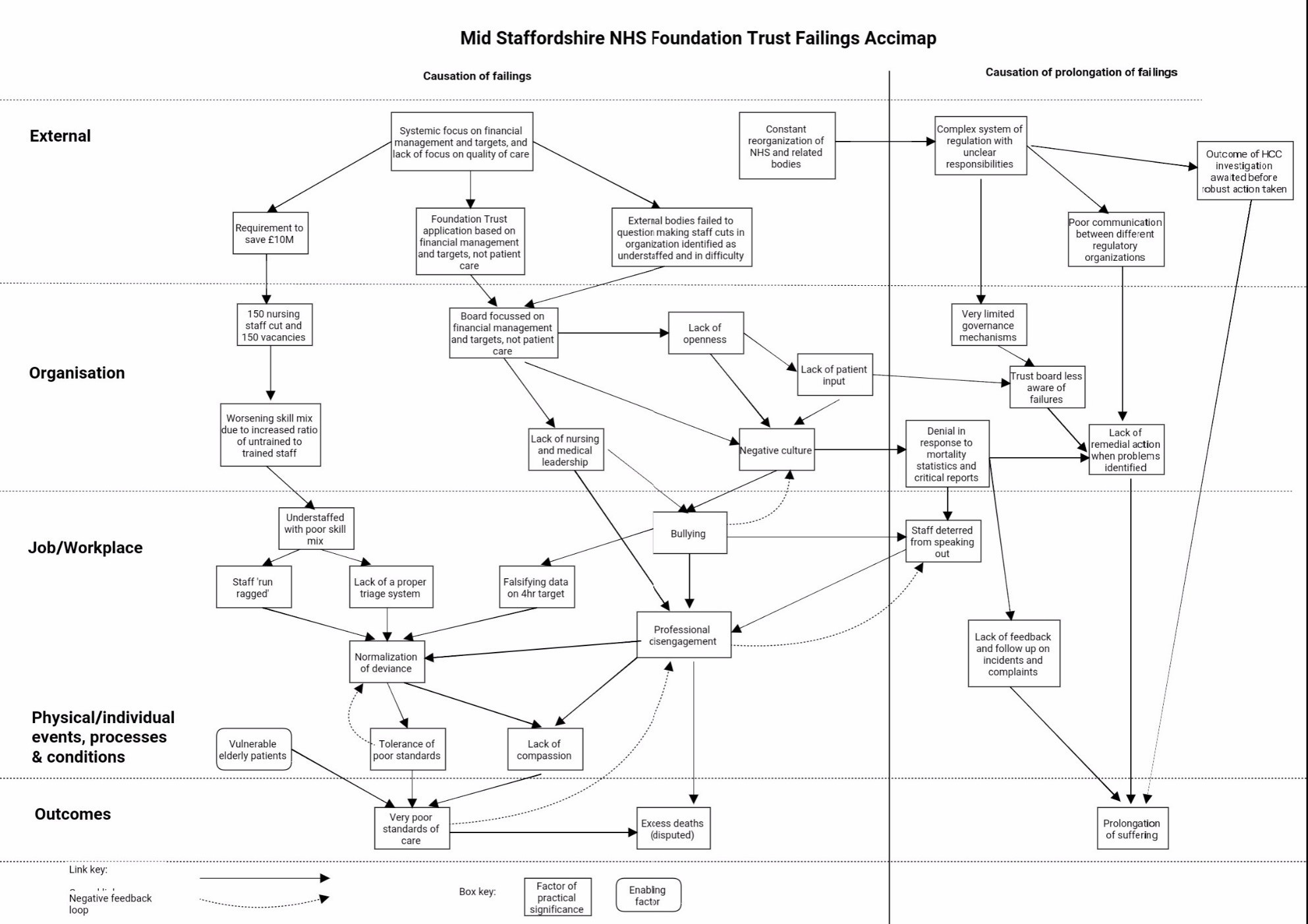
Failings at the Mid Staffordshire NHS Foundation Trust were described in the influential Francis report (2013). For this assignment, the data in the report was re-analysed using three different approaches; the Accimap, the Yorkshire Contributory Factors Framework and the Swiss Cheese Model. Each model provided different perspectives on the incident. The Accimap was the most useful for understanding the complex causation of the incident and is shown below:
Accimap of the Mid Staffordshire NHS Foundation Trust Failings
Healthcare Ergonomics and Patient Safety
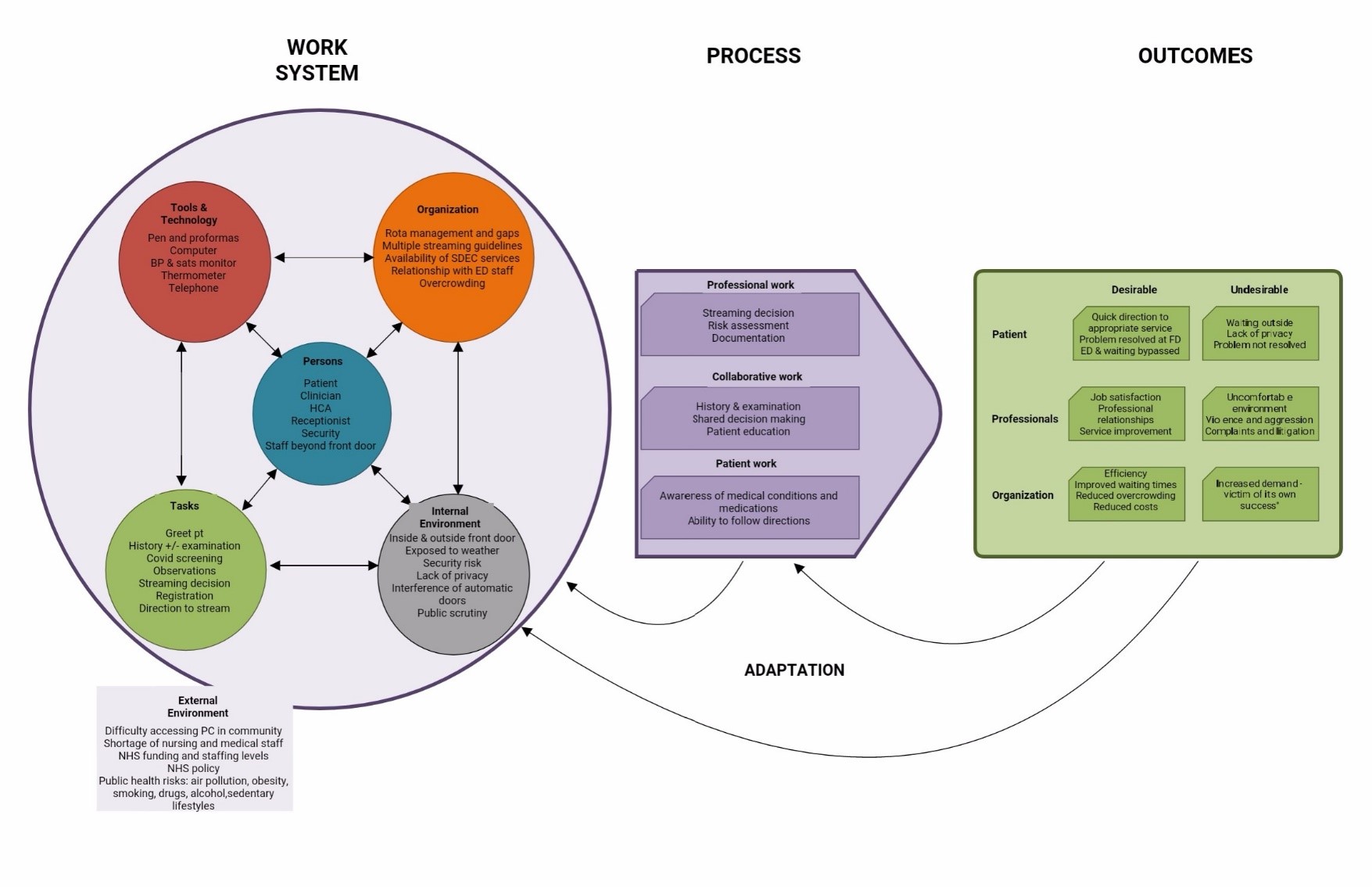
On arrival at the Urgent and Emergency Care Centre, patients are assessed at the front door to determine the best stream for their needs and their priority. This assignment analysed the process using two contrasting models. The Systems Engineering Initiative for Patient Safety (SEIPS) model proved useful for taking a comprehensive overview of all of the ergonomics and human factors issues at play and providing a clear graphical illustration. However, it only suggested improvement indirectly, by clarifying the issues. The Concepts for Applying Resilience Engineering (CARE) model was found to be less comprehensive, being focussed on resilience outcomes, and did not lend itself to a graphical representation of the system or recommendations. However, it gave much more detail on capacity, demand and adaptations and it gave detailed directions regarding making improvements with resilience outcomes. Overall, both models made a useful contribution to the understanding of the front door service as a system and suggested improvements to the physical environment, processes, staffing and information technology.
SEIPS model of the Urgent and Emergency Care Centre front door assessment process
Physical Ergonomics
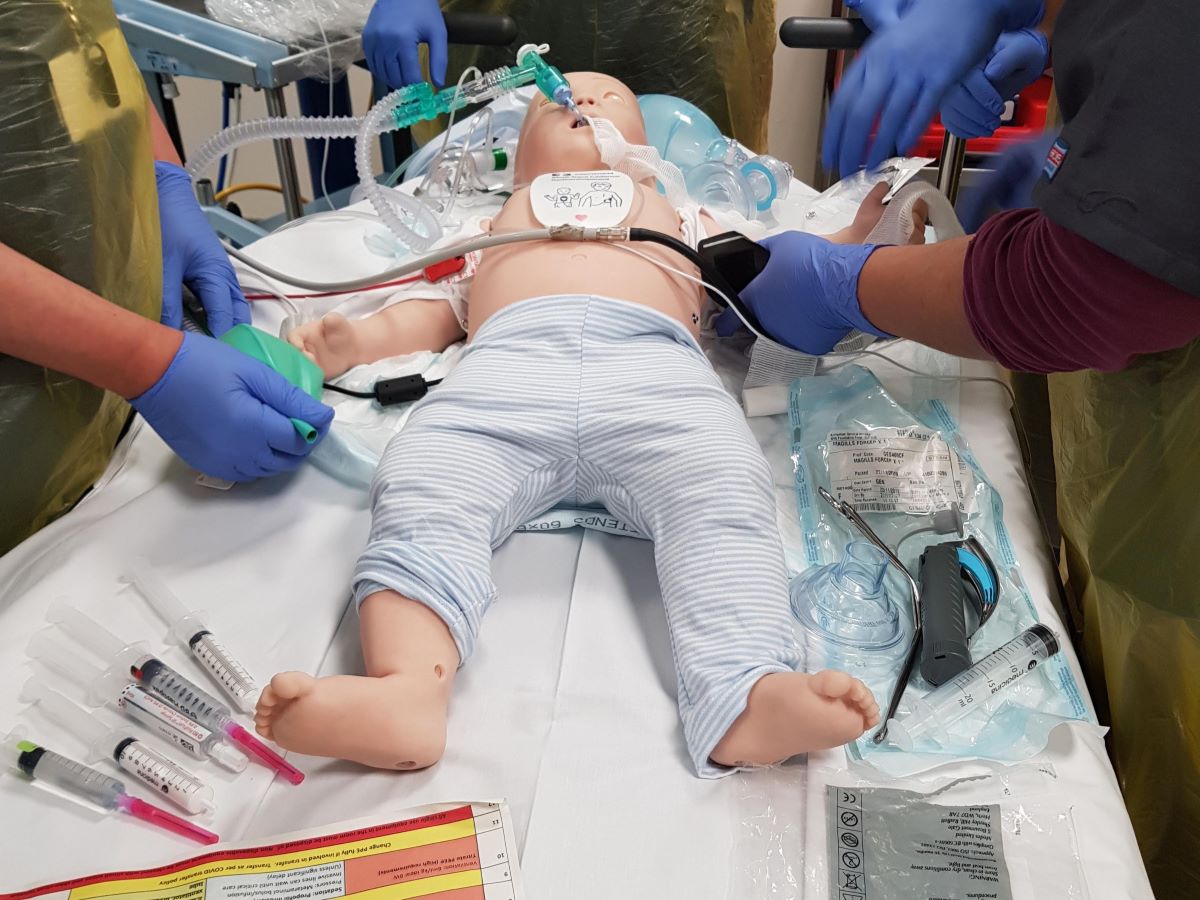
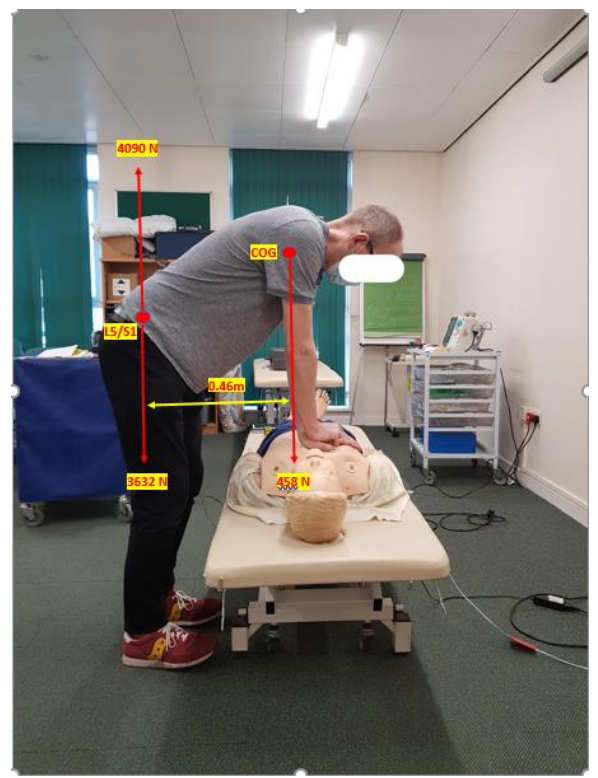
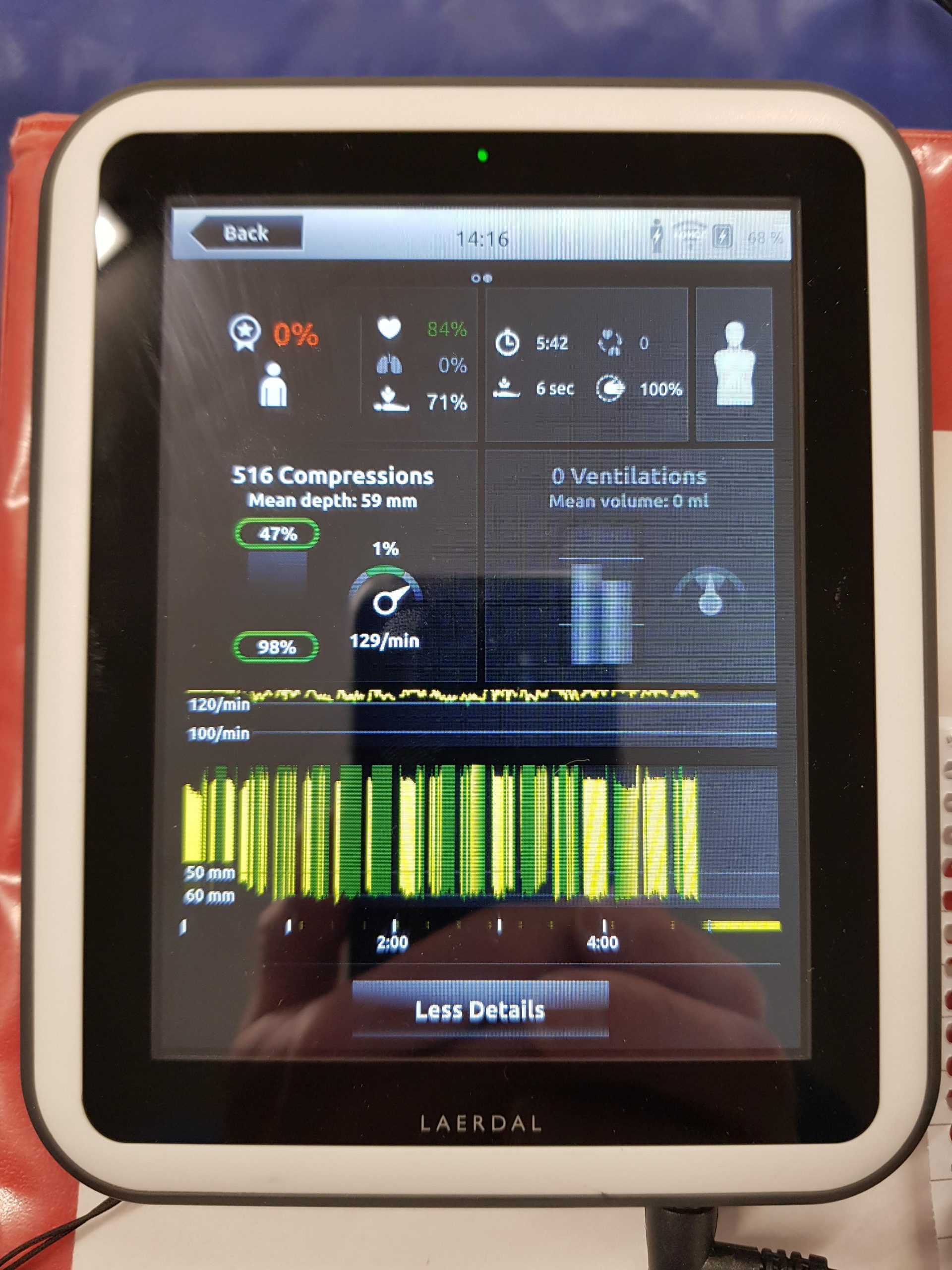
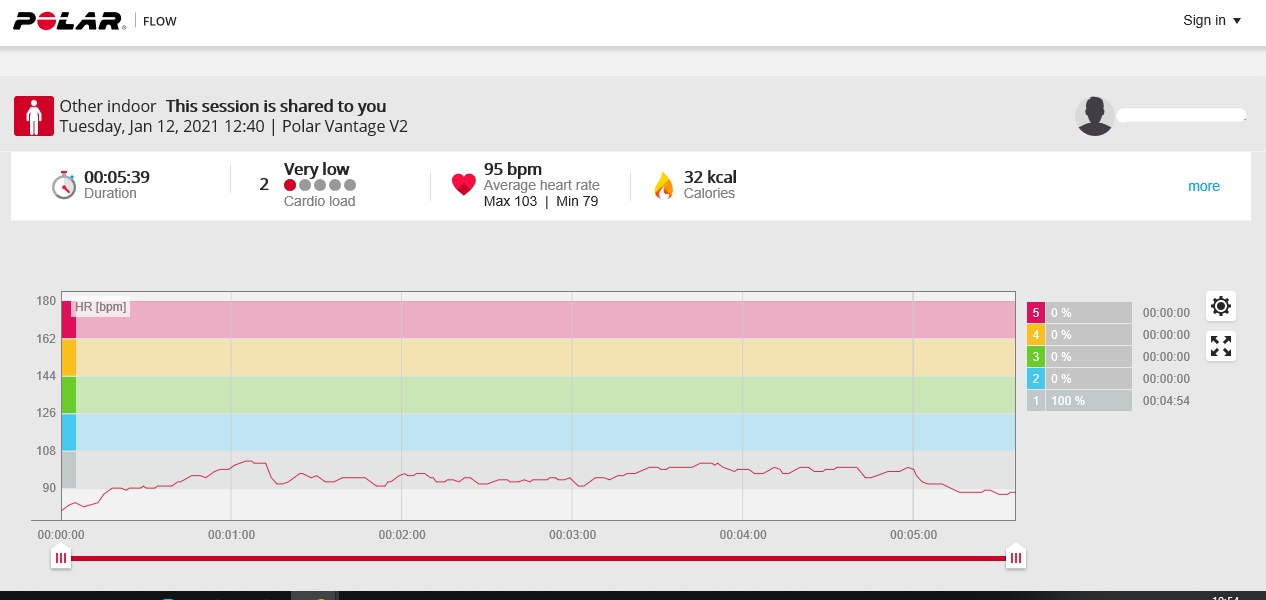
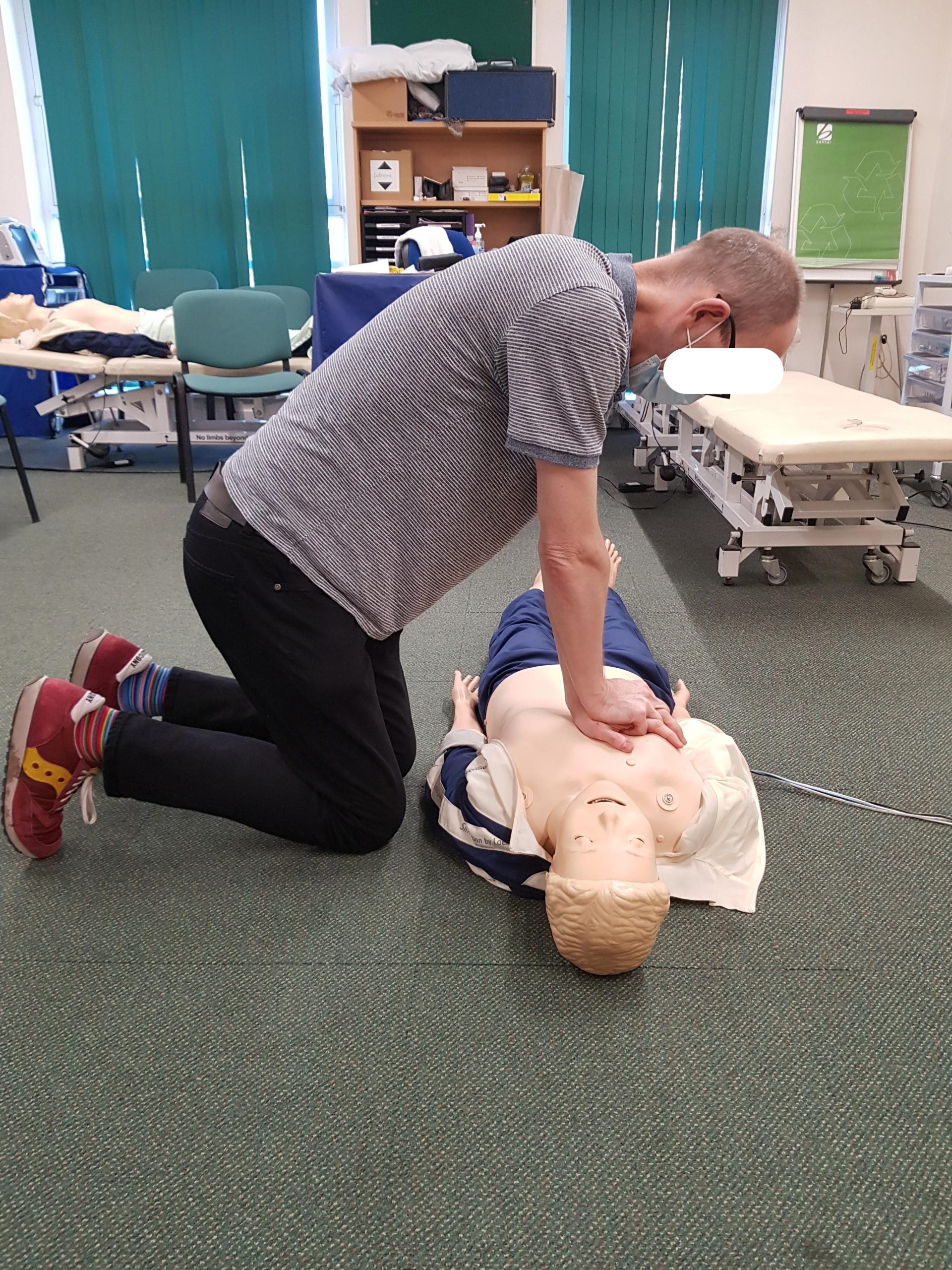
Cardiopulmonary Resuscitation (CPR) is a common practical procedure in healthcare that may cause injury to the operator or the patient and if performed sub optimally leads to worse outcomes. This assignment considered the task of CPR from the perspective of posture, physiology, biomechanics and anthropometry. Measurements and calculations were made on a single subject (see images below), but the implications for operators with different physical characteristics were discussed.
Photos: D. Stephenson
The postures required were classed as very high risk. Biomechanical analysis of a single recoil showed spinal compression force and frequency of compressions in excess of recommended guidelines. Chest compressions required a relatively low level of cardiovascular work, yet resulted in a higher perceived level of effort and evidence of rapid fatigue, leading to inadequate compressions. Considering the anthropometry related to CPR, low body weight and short stature will make it more difficult to produce adequate compressions, whilst high body weight and stature make it more difficult to allow full recoil. As a result, certain sized operators may be unable to provide adequate compressions or may fatigue very rapidly. The positioning of the patient on the floor, trolley or bed and the height and width variables of the workspace also make a significant contribution to the difficulty of achieving adequate compressions and recoil. Strategies for reducing the risk to the operator and improving the quality of CPR were discussed.
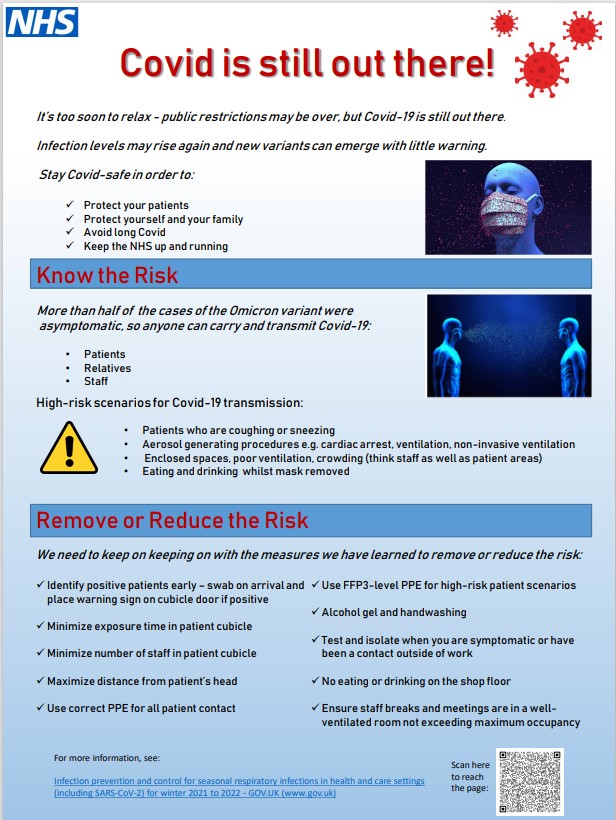
Occupational Ergonomics
This poster was produced to alert healthcare staff to the ongoing risk of COVID-19 infection in early 2022, when most restrictions had been lifted and there was a risk of complacency. It highlighted high-risk scenarios and suggested measures to reduce the risk.
Experience
I have over twenty years’ experience in Emergency Medicine. I have applied an ergonomics and human factors approach to many aspects of my work, such as incident investigation, quality improvement, simulation, electronic patient record projects and the design of new facilities and procedures. As I have gained new knowledge and skills from my MSc studies, I have been keen to put them into practice in my workplace. I submitted a log book of my experience to the Chartered Institute of Ergonomics and Human Factors in 2023 and was awarded Technical Membership (TechCIEHF).